
Bladder cancer represents one of the most biologically complex and clinically challenging malignancies in modern oncology. It is not merely a disease of uncontrolled cellular proliferation within the urinary bladder; rather, it is a multidimensional oncological condition shaped by environmental carcinogens, genetic mutations, immune dysregulation, occupational exposure, tobacco consumption, aging populations, and molecular heterogeneity. Across the world, bladder cancer continues to impose a major burden on healthcare systems because of its high recurrence rate, repeated need for surveillance, expensive treatment protocols, and profound impact on quality of life.
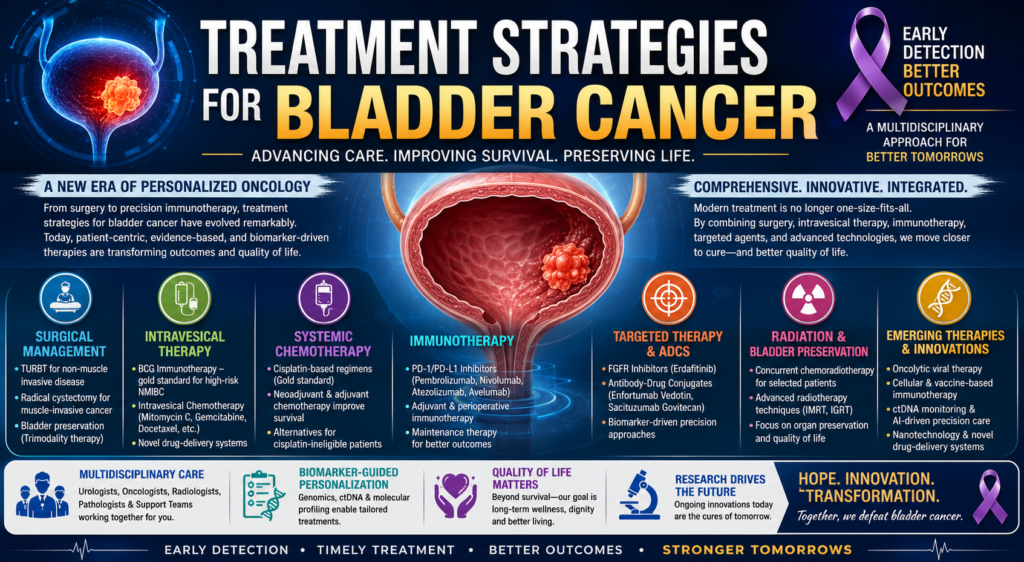
From a historical perspective, bladder cancer treatment was once dominated almost entirely by surgery. Radical cystectomy, urinary diversion, and palliative chemotherapy formed the backbone of therapy for decades. However, the landscape of bladder cancer management has undergone a revolutionary transformation in recent years. The emergence of precision medicine, molecular oncology, immunotherapy, antibody-drug conjugates, targeted therapies, bladder-preservation strategies, and biomarker-driven treatment protocols has dramatically altered therapeutic decision-making. The modern clinician is no longer confined to choosing between surgery and chemotherapy alone. Today’s bladder cancer treatment paradigm is increasingly personalized, multidisciplinary, technologically sophisticated, and immunologically driven.
Globally, urothelial carcinoma accounts for nearly 90% of bladder cancer cases. Smoking remains the single most important risk factor and contributes significantly to disease incidence. Occupational exposure to aromatic amines, chronic inflammation, arsenic contamination, radiation exposure, and genetic susceptibility also contribute substantially to disease development. (Cancer.gov) The disease predominantly affects older adults and is more common in men than women. Yet despite advances in diagnostics and therapeutics, recurrence rates remain extraordinarily high, making bladder cancer one of the most expensive cancers to manage on a per-patient basis throughout a lifetime.
The therapeutic strategy for bladder cancer depends primarily upon disease staging. Broadly, bladder cancer is divided into non-muscle-invasive bladder cancer (NMIBC), muscle-invasive bladder cancer (MIBC), and metastatic bladder cancer. Each category represents a biologically distinct clinical entity requiring different therapeutic philosophies, risk stratification models, and long-term surveillance strategies.
Understanding the Biological Nature of Bladder Cancer
Before discussing treatment strategies, it is important to understand the biological behavior of bladder tumors. Unlike many solid tumors that exhibit linear progression, bladder cancer frequently demonstrates a dynamic cycle of recurrence, dormancy, progression, and clonal evolution. This biological unpredictability has historically complicated treatment planning.
Non-muscle-invasive tumors remain confined to the mucosa or lamina propria and are often managed through bladder-preserving approaches. However, these tumors possess a notorious tendency for recurrence. Studies indicate that recurrence rates may reach nearly 80% in certain high-risk groups. (Cancer.gov) More concerning is the possibility of progression toward muscle-invasive disease, which substantially worsens prognosis.
Muscle-invasive bladder cancer penetrates deeper layers of the bladder wall and carries a significantly higher risk of metastasis. Once metastatic dissemination occurs, survival outcomes historically declined dramatically. Yet modern systemic therapies are now altering survival trajectories in ways previously considered impossible.
The molecular landscape of bladder cancer has become increasingly important in therapeutic selection. Mutations involving FGFR3, TP53, RB1, PIK3CA, ERBB2, and DNA damage response pathways have opened new avenues for targeted treatment. Simultaneously, immune checkpoint biology involving PD-1 and PD-L1 has reshaped immunotherapeutic strategies in urothelial carcinoma. (PMC)
Surgical Management: The Historical Foundation of Bladder Cancer Treatment
Surgery remains one of the most important pillars of bladder cancer management. Despite remarkable advances in systemic therapies, surgical intervention continues to provide curative potential for localized disease.
Transurethral Resection of Bladder Tumor (TURBT)
For non-muscle-invasive bladder cancer, transurethral resection of bladder tumor serves as both a diagnostic and therapeutic procedure. Using cystoscopic instrumentation, visible tumors are resected from the bladder wall. TURBT allows pathological staging, grading, and risk assessment.
However, TURBT alone is often insufficient for long-term disease control because microscopic residual disease frequently persists. Consequently, intravesical therapies are commonly administered following resection to reduce recurrence and progression risk.
Repeat TURBT procedures may be necessary in high-grade tumors to ensure complete resection and accurate staging. This reflects the recurrent and multifocal biological behavior characteristic of urothelial carcinoma.
Radical Cystectomy
For muscle-invasive bladder cancer, radical cystectomy remains the gold standard curative approach in eligible patients. The surgery involves complete removal of the urinary bladder along with adjacent pelvic organs and lymph nodes. (Cancer.gov)
In men, the prostate and seminal vesicles are often removed, whereas women may undergo removal of the uterus, ovaries, fallopian tubes, anterior vaginal wall, and urethra. The procedure is technically demanding and associated with substantial physiological and psychological consequences.
Urinary diversion following cystectomy may involve:
- Ileal conduit diversion
- Continent cutaneous diversion
- Orthotopic neobladder reconstruction
The choice depends upon patient age, renal function, tumor location, performance status, and surgeon expertise.
Modern robotic-assisted radical cystectomy has improved perioperative precision and reduced blood loss, though long-term oncological superiority over open surgery remains debated.
Bladder Preservation Approaches
Not all patients are suitable candidates for radical cystectomy. Elderly individuals, medically frail patients, or those seeking organ preservation increasingly undergo trimodality therapy consisting of:
- Maximal TURBT
- Concurrent chemoradiotherapy
- Careful surveillance
Bladder preservation strategies have gained growing attention because of quality-of-life considerations. Emerging evidence suggests selected patients can achieve durable control while retaining bladder function. (Grand Rounds in Urology)
Intravesical Therapy: Localized Precision within the Bladder
Intravesical therapy revolutionized the management of non-muscle-invasive bladder cancer by allowing direct drug delivery into the bladder lumen.
Bacillus Calmette-Guérin (BCG) Immunotherapy
BCG remains one of the most remarkable examples of cancer immunotherapy in medical history. Derived from attenuated Mycobacterium bovis, BCG stimulates localized immune activation within the bladder microenvironment.
Rather than directly killing tumor cells like conventional chemotherapy, BCG activates innate and adaptive immune responses, recruiting macrophages, T lymphocytes, cytokines, and inflammatory mediators that target urothelial cancer cells. (Fox Chase Cancer Center)
BCG is especially effective in:
- High-risk NMIBC
- Carcinoma in situ
- Recurrent superficial tumors
Long-term studies demonstrate that BCG reduces progression risk and improves survival in selected patients. Yet approximately 30–40% of patients eventually develop BCG-unresponsive disease. (Bladder Cancer Canada)
This therapeutic limitation has driven intense global research toward next-generation intravesical immunotherapies and viral therapies.
Intravesical Chemotherapy
Agents such as mitomycin C, gemcitabine, epirubicin, and docetaxel are commonly instilled directly into the bladder following TURBT.
The rationale behind intravesical chemotherapy is simple yet powerful:
- achieve high local drug concentration
- minimize systemic toxicity
- reduce tumor recurrence
Combination intravesical regimens are increasingly being explored for BCG-refractory disease.
Systemic Chemotherapy: The Traditional Backbone of Advanced Disease
For decades, platinum-based chemotherapy represented the cornerstone of advanced bladder cancer management.
Cisplatin-Based Chemotherapy
Cisplatin-based combination regimens such as:
- MVAC (methotrexate, vinblastine, doxorubicin, cisplatin)
- Gemcitabine plus cisplatin
became standard therapies for muscle-invasive and metastatic disease.
Neoadjuvant chemotherapy administered before radical cystectomy significantly improves survival outcomes by eradicating micrometastatic disease. (Cancer.gov)
However, many patients remain ineligible for cisplatin because of:
- renal dysfunction
- hearing impairment
- poor performance status
- neuropathy
- advanced age
This clinical challenge accelerated the development of alternative systemic therapies.
Immunotherapy: The New Era of Bladder Cancer Treatment
Few developments in oncology have transformed bladder cancer care as profoundly as immune checkpoint inhibitors.
Bladder cancer is considered highly immunogenic because of its elevated mutational burden, making it particularly susceptible to immune-based therapies.
PD-1 and PD-L1 Inhibitors
Checkpoint inhibitors function by removing inhibitory signals that prevent T cells from attacking cancer cells.
Major approved agents include:
- Pembrolizumab
- Nivolumab
- Atezolizumab
- Avelumab
These therapies have dramatically altered treatment algorithms for advanced urothelial carcinoma. (PMC)
Pembrolizumab demonstrated survival benefits in platinum-refractory metastatic disease and is now widely integrated into therapeutic protocols.
Avelumab maintenance therapy after platinum chemotherapy has emerged as a major advancement by prolonging survival in responding patients. (Bladder Cancer Canada)
Adjuvant and Perioperative Immunotherapy
Modern research increasingly investigates immunotherapy in earlier disease stages.
Studies such as CheckMate 274 and NIAGARA demonstrated that perioperative immunotherapy can improve disease-free survival and overall outcomes in muscle-invasive bladder cancer. (Grand Rounds in Urology)
The integration of immunotherapy before and after surgery represents a paradigm shift in bladder cancer management.
Challenges of Immunotherapy
Despite extraordinary promise, immunotherapy faces important limitations:
- immune-related adverse effects
- variable response rates
- primary resistance
- acquired resistance
- biomarker uncertainty
Immune toxicities may involve:
- pneumonitis
- hepatitis
- endocrinopathies
- colitis
- dermatological reactions
Furthermore, only a subset of patients achieves durable long-term remission.
Consequently, ongoing research seeks predictive biomarkers including:
- PD-L1 expression
- tumor mutational burden
- ctDNA
- immune gene signatures
Targeted Therapy: Precision Oncology in Bladder Cancer
The rise of molecular oncology has enabled targeted therapeutic interventions based on specific genomic alterations.
FGFR Inhibitors
FGFR3 mutations are common in urothelial carcinoma, particularly in non-muscle-invasive disease.
Erdafitinib emerged as a landmark targeted therapy for patients with susceptible FGFR alterations. (UroToday)
The development of FGFR inhibitors represents the transition from histology-driven oncology toward biomarker-guided precision medicine.
Antibody-Drug Conjugates (ADCs)
Antibody-drug conjugates have become one of the most exciting frontiers in bladder cancer therapeutics.
These agents combine:
- monoclonal antibodies
- cytotoxic payloads
- tumor-specific targeting
Major ADCs include:
- Enfortumab Vedotin
- Sacituzumab Govitecan
Enfortumab vedotin targets nectin-4, a protein highly expressed in urothelial tumors. The therapy has shown remarkable efficacy in metastatic disease and increasingly appears in perioperative settings. (GU Oncology Now)
The combination of enfortumab vedotin with pembrolizumab is now reshaping frontline management for advanced bladder cancer.
Viral and Cellular Therapies
Emerging strategies include:
- oncolytic viral therapy
- cytokine-based immunotherapy
- engineered immune stimulators
Agents such as cretostimogene grenadenorepvec and nogapendekin alfa are under active investigation. (Cure Today)
These approaches seek not only tumor destruction but also durable immune memory formation.
Radiation Therapy and Chemoradiation
Radiotherapy continues to play a vital role in:
- bladder preservation
- palliation
- locally advanced disease
Concurrent chemoradiotherapy enhances radiosensitivity and improves local tumor control.
Modern radiation techniques such as:
- IMRT
- image-guided radiotherapy
- adaptive radiotherapy
have improved precision while minimizing toxicity to surrounding tissues.
For selected patients unwilling or unable to undergo cystectomy, trimodality therapy offers meaningful bladder preservation opportunities.
Personalized Medicine and Biomarker-Guided Therapy
The future of bladder cancer treatment increasingly depends upon molecular stratification.
Circulating Tumor DNA (ctDNA)
ctDNA represents one of the most promising innovations in precision oncology.
Minimal residual disease detection through ctDNA analysis may allow:
- early relapse prediction
- treatment intensification
- personalized surveillance
Recent studies suggest ctDNA-guided strategies may significantly refine postoperative treatment selection. (UroToday)
Molecular Subtyping
Bladder cancer is now recognized as comprising molecular subtypes analogous to breast cancer taxonomy:
- luminal subtype
- basal subtype
- neuroendocrine subtype
- immune-rich subtype
Each subtype exhibits distinct therapeutic responsiveness and biological behavior.
The integration of genomics into routine clinical care may ultimately individualize therapy at unprecedented levels.
Emerging Technologies in Bladder Cancer Management
The future of bladder cancer treatment lies at the intersection of oncology, biotechnology, artificial intelligence, molecular diagnostics, and precision therapeutics.
Artificial Intelligence
AI-driven pathology and radiology are improving:
- tumor detection
- recurrence prediction
- treatment planning
- prognostic modeling
Machine learning algorithms may soon guide personalized treatment decisions using integrated genomic and imaging datasets.
Drug Delivery Innovations
Novel intravesical drug-delivery platforms are being developed to improve drug retention and efficacy.
The TAR-200 intravesical system demonstrated highly encouraging clinical responses in BCG-unresponsive disease. (ecancer)
Sustained-release technologies may overcome limitations of conventional intravesical administration.
Nanotechnology
Nanomedicine-based drug delivery systems aim to:
- enhance tumor targeting
- reduce systemic toxicity
- improve intravesical penetration
- overcome drug resistance
Nanotechnology may eventually transform localized bladder cancer therapy.
Psychological and Quality-of-Life Dimensions
Bladder cancer treatment extends far beyond tumor eradication. Radical surgery, urinary diversion, chronic surveillance, sexual dysfunction, body-image alteration, and fear of recurrence profoundly affect psychological wellbeing.
Patients often experience:
- anxiety
- depression
- social isolation
- altered self-identity
Therefore, comprehensive bladder cancer management requires:
- psycho-oncology support
- rehabilitation
- nutritional guidance
- survivorship planning
- palliative care integration
Modern oncology increasingly recognizes that survival alone is insufficient without preservation of dignity and quality of life.
Challenges in Low- and Middle-Income Countries
In developing nations, bladder cancer care faces substantial barriers:
- limited access to immunotherapy
- high treatment costs
- inadequate diagnostic infrastructure
- shortage of trained uro-oncologists
- poor awareness
- delayed diagnosis
In India and many resource-constrained regions, affordability remains a major determinant of therapeutic accessibility.
Precision oncology promises scientific advancement, but healthcare inequity threatens to widen global disparities unless cost-effective delivery systems and public healthcare reforms accompany technological progress.
The Future of Bladder Cancer Treatment
Bladder cancer therapy is entering a transformative era characterized by:
- precision immunotherapy
- antibody-drug conjugates
- molecular diagnostics
- bladder preservation
- adaptive treatment algorithms
- biomarker-driven personalization
The future treatment model will likely involve:
- genomic profiling at diagnosis
- dynamic ctDNA monitoring
- AI-assisted risk prediction
- individualized immunotherapy combinations
- minimally invasive interventions
- organ preservation whenever feasible
Research pipelines increasingly focus on:
- overcoming immunotherapy resistance
- improving predictive biomarkers
- combining ADCs with checkpoint inhibitors
- vaccine-based therapies
- cellular immunotherapy
- microbiome modulation
The philosophy of bladder cancer management is gradually shifting from aggressive anatomical removal toward biologically intelligent disease control.
Conclusion
The treatment landscape of bladder cancer has evolved from a predominantly surgical discipline into one of the most scientifically dynamic areas of modern oncology. Today, bladder cancer management integrates surgery, immunology, molecular biology, genomics, radiotherapy, biotechnology, and precision medicine into an increasingly sophisticated therapeutic ecosystem.
Radical cystectomy continues to offer curative potential for localized invasive disease, yet bladder-preserving approaches are gaining momentum through advances in chemoradiation and immunotherapy. Intravesical BCG remains historically significant, while immune checkpoint inhibitors have fundamentally redefined systemic therapy. Targeted therapies and antibody-drug conjugates now provide new hope for patients previously facing limited options.
The future of bladder cancer treatment will not be defined merely by stronger drugs or more aggressive surgery. Instead, it will be defined by precision — understanding the molecular identity of each tumor, the immunological profile of each patient, and the biological mechanisms underlying resistance and recurrence.
Bladder cancer management is becoming increasingly personalized, multidisciplinary, and patient-centered. As precision oncology continues to mature, the possibility of transforming bladder cancer from a recurrent and lethal malignancy into a controllable chronic disease becomes increasingly realistic.
The next generation of bladder cancer therapy will likely be guided not only by tumor stage but by genomic intelligence, immunological profiling, artificial intelligence, and adaptive therapeutic algorithms. In this evolving landscape, the ultimate objective is not simply prolonged survival, but preservation of human dignity, organ function, psychological wellbeing, and quality of life.