
Breast cancer stands among the most scientifically studied yet biologically complex diseases in modern medicine. It is not simply a malignancy of breast tissue; rather, it represents a multidimensional molecular disorder involving genetic instability, hormonal dysregulation, aberrant intracellular signaling pathways, immune evasion, metabolic adaptation, and tumor microenvironment remodeling. Across centuries, breast cancer has profoundly shaped the history of surgery, oncology, endocrinology, pharmacology, radiation science, molecular biology, and precision medicine. The journey of breast cancer treatment reflects humanity’s broader struggle against cancer itself — a progression from superstition and radical anatomical destruction toward molecularly guided, patient-centered, precision therapeutics.
Historically, breast cancer was feared as an incurable and fatal disease associated with pain, social stigma, disfigurement, and inevitable mortality. Ancient physicians observed breast tumors but lacked scientific understanding regarding their origin or biological behavior. Today, however, breast cancer treatment represents one of the most advanced and personalized fields in oncology, integrating genomics, immunotherapy, targeted therapeutics, biomarker-driven medicine, artificial intelligence, nanotechnology, and systems biology.
The transformation of breast cancer treatment over the last century is one of the greatest achievements in medical science. Survival rates have improved dramatically because of advances in early detection, surgical refinement, radiation therapy, endocrine manipulation, systemic chemotherapy, monoclonal antibodies, antibody-drug conjugates, CDK inhibitors, PARP inhibitors, immunotherapy, and molecular diagnostics. Yet despite these advancements, breast cancer remains a major global public health challenge, affecting millions of women annually and increasingly impacting younger populations in both developed and developing nations.
Modern breast cancer is no longer viewed as a single disease. Instead, it is recognized as a heterogeneous collection of molecularly distinct subtypes characterized by unique signaling pathways, receptor expression profiles, mutational landscapes, therapeutic vulnerabilities, and prognostic patterns. The contemporary era of breast oncology is therefore defined by precision medicine — understanding not only where the tumor is located anatomically, but how it behaves biologically at the molecular level.
Historical Evolution of Breast Cancer Treatment
The history of breast cancer treatment dates back thousands of years. Ancient Egyptian medical texts such as the Edwin Smith Papyrus described breast tumors as incurable masses treated with cauterization. At that time, disease was often interpreted through mystical or spiritual frameworks rather than scientific pathology.
Greek physicians including Hippocrates proposed that cancer resulted from an imbalance of bodily humors, particularly excess black bile. The term “cancer” itself emerged from the Greek word karkinos, describing the crab-like appearance of advanced tumors.
For centuries, breast cancer remained largely untreatable. Surgical interventions were crude, painful, and frequently fatal because anesthesia, antisepsis, and modern surgical techniques had not yet developed. Most patients died from infection, hemorrhage, or metastatic progression.
A major turning point occurred during the nineteenth century with the emergence of modern surgery. William Halsted introduced the radical mastectomy in the late 1800s, revolutionizing breast cancer management. The procedure involved extensive removal of:
- breast tissue
- pectoral muscles
- axillary lymph nodes
Halsted believed breast cancer spread in a stepwise anatomical manner. Radical surgery therefore aimed to eliminate local disease aggressively before metastasis occurred.
For decades, radical mastectomy became the dominant treatment philosophy worldwide. Although effective in some patients, the procedure often caused profound physical deformity and psychological trauma.
The twentieth century witnessed gradual shifts away from extreme surgical mutilation toward more conservative approaches. Clinical trials eventually demonstrated that breast-conserving surgery combined with radiation therapy could achieve survival outcomes comparable to radical mastectomy in selected patients.
This marked the beginning of modern multidisciplinary breast oncology.
The Molecular Revolution in Breast Cancer
The most profound transformation in breast cancer treatment emerged from advances in molecular biology and receptor science.
Scientists discovered that breast tumors differ biologically based upon receptor expression:
- Estrogen receptor (ER)
- Progesterone receptor (PR)
- Human epidermal growth factor receptor 2 (HER2)
These discoveries fundamentally altered therapeutic strategies.
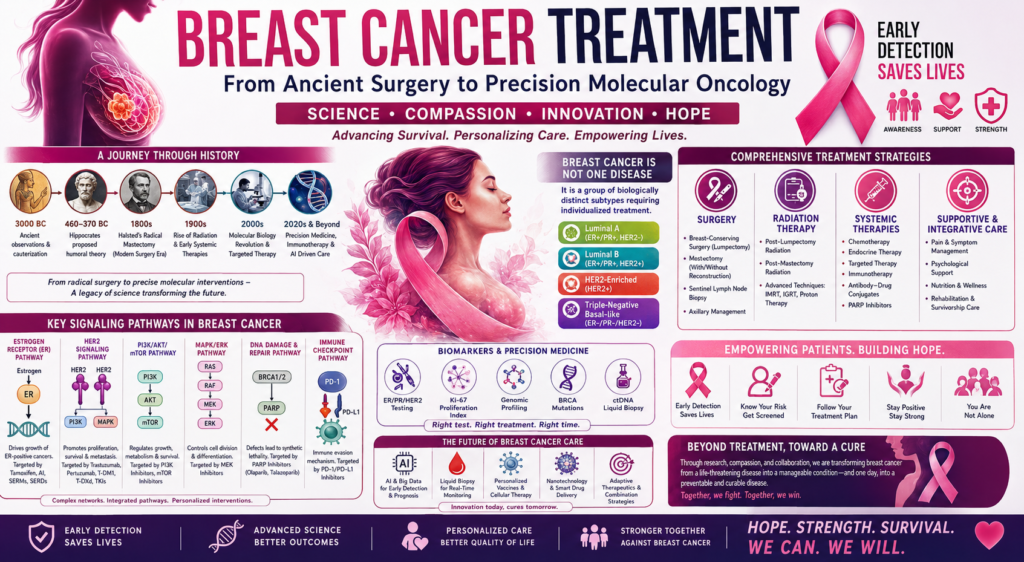
Breast cancer gradually became categorized into molecular subtypes:
- Luminal A
- Luminal B
- HER2-enriched
- Triple-negative breast cancer (TNBC)
Each subtype possesses distinct signaling pathways, growth kinetics, metastatic behavior, and treatment responsiveness.
The modern era therefore shifted oncology away from purely anatomical classification toward molecular oncology.
Surgical Treatment Strategies in Modern Breast Cancer
Despite major systemic advances, surgery remains a foundational pillar of breast cancer treatment.
Breast-Conserving Surgery
Breast-conserving surgery, also known as lumpectomy or partial mastectomy, involves removal of the tumor with preservation of surrounding breast tissue.
This approach offers several advantages:
- improved cosmetic outcomes
- reduced psychological burden
- preservation of body image
- equivalent survival in selected patients
Radiotherapy is usually administered postoperatively to minimize local recurrence risk.
Mastectomy
Mastectomy remains necessary in:
- multicentric tumors
- extensive disease
- inflammatory breast cancer
- BRCA mutation carriers
- recurrent disease
Modern mastectomy techniques increasingly emphasize reconstructive surgery and aesthetic preservation.
Sentinel Lymph Node Biopsy
Historically, extensive axillary lymph node dissection caused substantial morbidity including:
- lymphedema
- neuropathy
- shoulder dysfunction
Sentinel lymph node biopsy revolutionized surgical staging by minimizing unnecessary nodal dissection while maintaining diagnostic accuracy.
Radiation Therapy in Breast Cancer
Radiation therapy evolved dramatically during the twentieth century.
Initially used primarily for palliation, radiotherapy now plays critical roles in:
- breast conservation
- post-mastectomy management
- regional nodal control
- metastatic symptom relief
Modern radiotherapy techniques include:
- intensity-modulated radiation therapy (IMRT)
- image-guided radiotherapy
- proton therapy
- accelerated partial breast irradiation
These technologies improve tumor targeting while reducing cardiac and pulmonary toxicity.
Endocrine Therapy: Hormonal Manipulation in Breast Cancer
One of the most important milestones in breast oncology was recognition of hormonal dependence in many breast tumors.
Estrogen Signaling Pathway
The estrogen receptor signaling pathway represents a central driver in ER-positive breast cancer.
When estrogen binds to estrogen receptors:
- receptor dimerization occurs
- nuclear translocation follows
- transcriptional activation stimulates cell proliferation
ER-positive tumors depend heavily on this pathway for growth and survival.
Tamoxifen
Tamoxifen revolutionized breast cancer treatment by acting as a selective estrogen receptor modulator (SERM).
The drug competitively inhibits estrogen receptor activation within breast tissue, thereby suppressing tumor proliferation.
Tamoxifen significantly reduced:
- recurrence rates
- contralateral breast cancer risk
- mortality
Its development transformed endocrine oncology permanently.
Aromatase Inhibitors
Postmenopausal women primarily produce estrogen through peripheral aromatization.
Aromatase inhibitors including:
- anastrozole
- letrozole
- exemestane
block estrogen synthesis and became superior alternatives in many postmenopausal patients.
CDK4/6 Pathway and Inhibitors
The cyclin D–CDK4/6–RB signaling pathway plays a major role in cell-cycle progression.
In ER-positive breast cancer:
- estrogen signaling activates cyclin D
- cyclin D stimulates CDK4/6
- RB phosphorylation permits G1-S cell-cycle transition
CDK4/6 inhibitors including:
- palbociclib
- ribociclib
- abemaciclib
dramatically improved progression-free survival in metastatic ER-positive disease.
The CDK4/6 pathway represents one of the most important modern therapeutic targets in breast oncology.
HER2 Signaling Pathway and Targeted Therapy
HER2-positive breast cancer historically carried poor prognosis because of aggressive tumor biology.
HER2 receptor overexpression activates multiple downstream pathways:
- PI3K/AKT/mTOR pathway
- RAS/RAF/MEK/ERK pathway
- MAPK signaling
These signaling cascades stimulate:
- cellular proliferation
- angiogenesis
- metastasis
- apoptosis resistance
Trastuzumab: A Historic Breakthrough
Trastuzumab, a monoclonal antibody targeting HER2 receptors, revolutionized breast cancer therapy.
Mechanisms include:
- HER2 receptor blockade
- antibody-dependent cellular cytotoxicity
- inhibition of downstream signaling
The introduction of trastuzumab dramatically improved survival outcomes.
Advanced HER2 Therapies
Modern HER2-targeted therapies include:
- pertuzumab
- trastuzumab emtansine (T-DM1)
- trastuzumab deruxtecan
- tucatinib
- lapatinib
Antibody-drug conjugates represent particularly important innovations because they combine targeted specificity with cytotoxic payload delivery.
PI3K/AKT/mTOR Signaling Pathway
The PI3K/AKT/mTOR pathway is among the most critical intracellular signaling networks in breast cancer.
This pathway regulates:
- metabolism
- protein synthesis
- survival
- proliferation
- angiogenesis
PIK3CA mutations commonly occur in hormone receptor-positive tumors.
Targeted therapies such as alpelisib inhibit PI3K signaling and improve outcomes in selected patients.
mTOR inhibitors including everolimus also suppress downstream pathway activation.
Triple-Negative Breast Cancer: The Most Challenging Subtype
Triple-negative breast cancer lacks:
- estrogen receptors
- progesterone receptors
- HER2 expression
This subtype demonstrates:
- aggressive behavior
- early metastasis
- genomic instability
- limited targeted options
Historically, chemotherapy remained the primary treatment modality.
However, modern molecular insights are transforming TNBC management.
BRCA Signaling and PARP Inhibitors
BRCA1 and BRCA2 genes are essential for homologous recombination DNA repair.
BRCA mutations impair DNA repair capacity, rendering tumors vulnerable to PARP inhibition.
PARP inhibitors including:
- olaparib
- talazoparib
induce synthetic lethality in BRCA-mutated cancers.
This represents a major triumph of precision oncology.
Immune Checkpoint Pathways
TNBC frequently exhibits:
- high mutational burden
- immune infiltration
- PD-L1 expression
Checkpoint inhibitors targeting:
- PD-1
- PD-L1
have demonstrated important therapeutic activity.
Agents such as pembrolizumab and atezolizumab are increasingly integrated into TNBC management.
Chemotherapy in Breast Cancer
Despite targeted therapy advancements, chemotherapy remains essential across many disease settings.
Major classes include:
- anthracyclines
- taxanes
- alkylating agents
- antimetabolites
- platinum compounds
Chemotherapy mechanisms involve:
- DNA damage
- mitotic inhibition
- apoptosis induction
Neoadjuvant chemotherapy allows:
- tumor downstaging
- breast conservation
- response assessment
Pathological complete response has emerged as an important prognostic indicator, particularly in HER2-positive and triple-negative disease.
Tumor Microenvironment and Immune Biology
Modern breast cancer research increasingly emphasizes the tumor microenvironment.
Tumors interact dynamically with:
- fibroblasts
- immune cells
- extracellular matrix
- cytokines
- angiogenic factors
VEGF Signaling Pathway
The vascular endothelial growth factor pathway drives tumor angiogenesis.
VEGF stimulates:
- endothelial proliferation
- vascular permeability
- neovascularization
Anti-angiogenic therapies attempt to disrupt tumor blood supply, though benefits in breast cancer remain variable.
NF-kB Signaling Pathway
NF-kB regulates inflammatory signaling and contributes to:
- metastasis
- immune suppression
- apoptosis resistance
Chronic inflammatory signaling may facilitate tumor progression and therapeutic resistance.
Metastatic Breast Cancer: Evolution of Long-Term Disease Management
Metastatic breast cancer was once considered rapidly fatal.
Today, advances in systemic therapy increasingly allow prolonged disease control.
Modern management involves:
- sequential targeted therapy
- endocrine combinations
- immunotherapy
- ADCs
- precision molecular profiling
The treatment philosophy has evolved from purely palliative care toward chronic disease management.
Antibody-Drug Conjugates: A New Therapeutic Era
ADCs represent one of the most exciting innovations in modern breast oncology.
These therapies combine:
- monoclonal antibodies
- linker technologies
- cytotoxic agents
Examples include:
- trastuzumab deruxtecan
- sacituzumab govitecan
ADCs improve therapeutic specificity while minimizing systemic toxicity.
Signaling Pathways Involved in Breast Cancer Progression and Treatment
Breast cancer progression involves interconnected molecular signaling networks.
Major pathways include:
Estrogen Receptor Pathway
Controls hormone-dependent proliferation.
HER2/EGFR Pathway
Activates proliferation and survival signaling.
PI3K/AKT/mTOR Pathway
Promotes metabolism, growth, and therapeutic resistance.
RAS/RAF/MEK/ERK Pathway
Regulates proliferation and differentiation.
JAK/STAT Pathway
Involved in cytokine signaling and immune modulation.
Wnt/Beta-Catenin Pathway
Contributes to stemness and metastasis.
Hedgehog Signaling Pathway
Associated with tumor initiation and resistance.
Notch Signaling Pathway
Regulates cell fate determination and cancer stem cells.
TGF-Beta Pathway
Promotes epithelial–mesenchymal transition and metastasis.
Apoptotic Pathways
Dysregulation permits cancer cell survival.
These pathways do not function independently. Instead, breast cancer biology reflects extensive signaling cross-talk and adaptive resistance mechanisms.
Resistance Mechanisms in Breast Cancer
Therapeutic resistance remains one of the greatest challenges in oncology.
Mechanisms include:
- receptor mutations
- pathway redundancy
- clonal evolution
- immune escape
- tumor heterogeneity
- epithelial–mesenchymal transition
Understanding resistance biology is essential for developing next-generation therapies.
Artificial Intelligence and Precision Oncology
AI is increasingly transforming breast cancer management through:
- radiological interpretation
- digital pathology
- genomic analysis
- risk prediction
- treatment optimization
Machine learning may eventually personalize therapy in real time based on dynamic molecular changes.
Nanotechnology and Drug Delivery
Nanomedicine seeks to improve:
- tumor targeting
- drug penetration
- pharmacokinetics
- toxicity reduction
Nanoparticle-based therapeutics may redefine systemic cancer therapy in the future.
Psychological and Social Dimensions of Breast Cancer
Breast cancer affects far more than physiology alone.
Patients frequently experience:
- anxiety
- depression
- fear of recurrence
- altered femininity
- body image disturbance
- social stigma
Modern oncology increasingly integrates:
- psycho-oncology
- survivorship care
- rehabilitation
- fertility preservation
- sexual health counseling
Human dignity and quality of life are now central components of cancer care.
Global Challenges and Healthcare Inequity
Despite scientific progress, substantial disparities remain worldwide.
In low- and middle-income countries:
- delayed diagnosis
- limited screening
- poor access to targeted therapy
- financial toxicity
- inadequate oncology infrastructure
continue to compromise outcomes.
Global oncology must therefore balance scientific innovation with accessibility and affordability.
Future Directions in Breast Cancer Treatment
The future of breast oncology lies in:
- liquid biopsy
- ctDNA monitoring
- adaptive therapeutics
- personalized vaccines
- cellular therapy
- AI-driven oncology
- epigenetic therapeutics
- microbiome modulation
Treatment strategies increasingly seek not merely tumor eradication, but intelligent biological control.
Conclusion
The history of breast cancer treatment reflects one of humanity’s most extraordinary scientific transformations. What began centuries ago as a poorly understood and surgically mutilating disease has evolved into a sophisticated molecular oncology discipline driven by precision medicine, targeted therapeutics, immunology, and systems biology.
Modern breast cancer treatment is no longer defined solely by tumor size or anatomical staging. Instead, it is guided by receptor biology, signaling pathways, genomic alterations, immune landscapes, and molecular heterogeneity. Surgical management remains foundational, yet endocrine therapy, HER2-directed therapy, CDK4/6 inhibition, PARP inhibition, immunotherapy, and antibody-drug conjugates have fundamentally reshaped therapeutic outcomes.
The understanding of signaling pathways such as:
- ER signaling
- HER2 signaling
- PI3K/AKT/mTOR
- MAPK
- JAK/STAT
- Wnt
- Notch
- TGF-beta
has revolutionized therapeutic targeting and enabled precision oncology.
The future of breast cancer management will likely depend upon integration of:
- molecular diagnostics
- real-time genomic monitoring
- AI-assisted decision-making
- individualized therapeutics
- immunological engineering
Breast cancer treatment is increasingly transitioning from generalized chemotherapy toward biologically intelligent intervention. The ultimate objective is no longer merely extending survival, but preserving dignity, quality of life, psychological wellbeing, reproductive health, and long-term survivorship.
As oncology enters the age of precision medicine, breast cancer stands as one of the clearest examples of how molecular science, pharmacology, immunology, and human resilience together can transform the destiny of disease itself.