
Introduction
Urinary tract infections (UTIs) represent one of the most common infectious diseases affecting humanity. Despite being historically categorized as “routine bacterial infections,” UTIs have now emerged as a major global healthcare challenge involving antimicrobial resistance, recurrent disease burden, hospital-acquired infections, biofilm biology, healthcare economics, women’s health, aging populations, and precision infectious disease medicine.
Every year, hundreds of millions of individuals worldwide suffer from UTIs, making them among the leading causes of outpatient antibiotic prescriptions and hospital antimicrobial utilization. Women are disproportionately affected due to anatomical and hormonal factors, although UTIs also represent major healthcare concerns among elderly individuals, diabetic patients, catheterized patients, immunocompromised populations, and critically ill hospitalized patients.
Modern medicine is witnessing a dramatic transformation in the epidemiology and management of UTIs. Rising multidrug-resistant (MDR) uropathogens, increasing resistance against fluoroquinolones and cephalosporins, recurrent infections, catheter-associated urinary tract infections (CAUTIs), and biofilm-associated microbial persistence are reshaping therapeutic strategies worldwide.
Recent WHO antimicrobial resistance surveillance reports reveal alarming resistance rates among major UTI pathogens such as Escherichia coli and Klebsiella pneumoniae, particularly against third-generation cephalosporins and fluoroquinolones. (World Health Organization)
Simultaneously, the field of UTI therapeutics is entering a new era characterized by:
- Novel antibiotics
- Precision diagnostics
- AI-assisted resistance prediction
- Microbiome-based therapies
- Vaccines
- Phage therapy
- Immunomodulation
- Antimicrobial stewardship frameworks
One of the most important recent developments was the approval of gepotidacin (Blujepa), the first new oral antibiotic class for uncomplicated UTIs in nearly three decades. (Sharp HealthCare)
Thus, urinary tract infections are no longer merely localized bacterial diseases. They have become strategic indicators of the broader global crisis involving microbial evolution, antibiotic resistance, healthcare infrastructure, and pharmaceutical innovation.
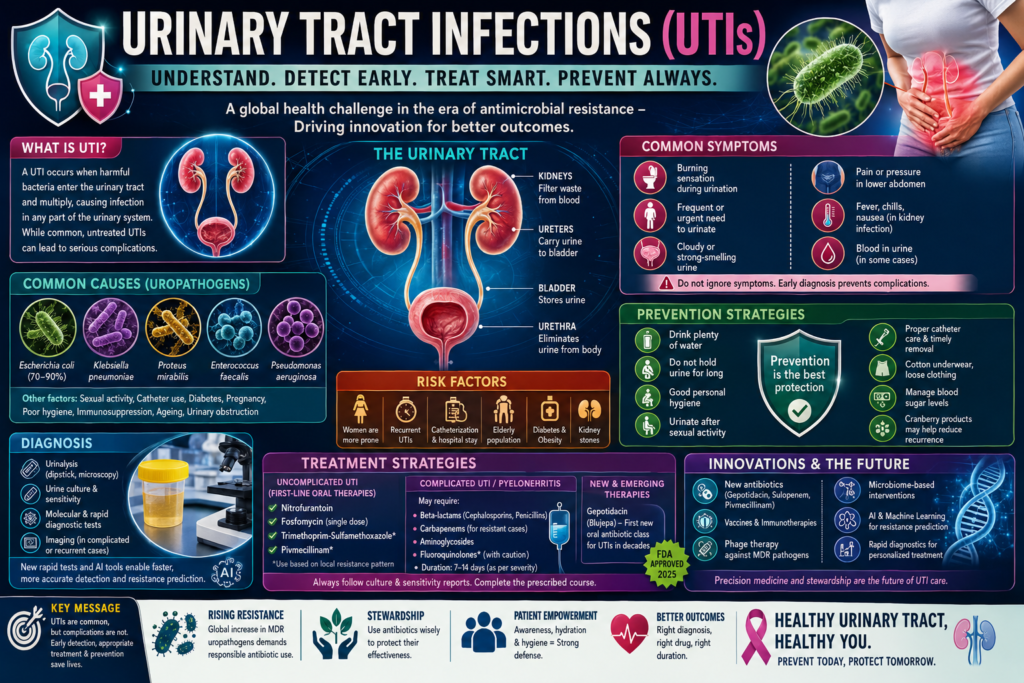
Understanding the Urinary Tract and Infection Pathogenesis
The urinary tract consists of:
- Kidneys
- Ureters
- Bladder
- Urethra
Under normal physiological conditions, the urinary tract maintains sterility through multiple defense mechanisms:
- Continuous urine flow
- Acidic urinary environment
- Mucosal immunity
- Antimicrobial peptides
- Normal microbiota interactions
UTIs develop when pathogenic microorganisms overcome these protective barriers and colonize urinary tissues.
The majority of UTIs occur through ascending infection:
- Periurethral colonization
- Urethral entry
- Bladder invasion
- Potential renal ascent
The bacterial growth concept may be represented as:
N_t = N_0 e^{\mu t}
where:
- (N_t) = bacterial population over time
- (N_0) = initial inoculum
- (\mu) = microbial growth rate
The rapid multiplication of bacteria within the urinary tract leads to inflammation, tissue injury, and clinical symptoms.
Epidemiology of UTIs
UTIs remain among the most prevalent bacterial infections globally.
Epidemiological estimates indicate:
- Over 50% of women experience at least one UTI during life
- Approximately 20–30% develop recurrent infections
- Millions of hospitalizations occur annually due to complicated UTIs
Recent analyses highlight escalating global UTI burden alongside increasing antimicrobial resistance. (MDPI)
Women are particularly vulnerable due to:
- Short urethra
- Hormonal influences
- Sexual activity
- Pregnancy-related physiological changes
Other high-risk populations include:
- Elderly individuals
- Diabetic patients
- Catheterized patients
- ICU patients
- Renal transplant recipients
India and other low- and middle-income countries face particularly severe UTI challenges due to:
- High antibiotic misuse
- Inadequate diagnostics
- Hospital overcrowding
- Catheter-associated infections
- Poor antimicrobial stewardship
Classification of UTIs
Modern clinical medicine classifies UTIs into several major categories.
Uncomplicated UTIs
These occur in otherwise healthy individuals with structurally normal urinary tracts.
Examples:
- Acute cystitis
- Simple lower urinary tract infections
Complicated UTIs (cUTIs)
Complicated UTIs involve:
- Structural abnormalities
- Urinary obstruction
- Catheterization
- Immunocompromised states
- Renal involvement
These infections carry higher risks of:
- Treatment failure
- Resistance
- Sepsis
- Recurrence
Recent IDSA and EAU guideline updates increasingly focus on optimized management of complicated UTIs amid rising resistance. (IDSA)
Recurrent UTIs
Defined as:
- ≥2 infections within 6 months
or - ≥3 infections within 1 year
Recurrent UTIs represent one of the most difficult clinical and quality-of-life challenges in modern urology and infectious disease medicine.
Catheter-Associated UTIs (CAUTIs)
CAUTIs remain among the most common hospital-acquired infections globally.
Biofilm formation on catheter surfaces significantly complicates treatment.
Microbiology of UTIs
Escherichia coli: The Dominant Uropathogen
Uropathogenic Escherichia coli (UPEC) causes approximately 70–90% of community-acquired UTIs.
Key virulence factors include:
- Fimbriae
- Adhesins
- Biofilm formation
- Iron acquisition systems
- Toxins
UPEC attaches to urothelial cells and evades immune clearance.
Other Important Uropathogens
Other organisms include:
- Klebsiella pneumoniae
- Proteus mirabilis
- Enterococcus faecalis
- Pseudomonas aeruginosa
- Staphylococcus saprophyticus
Hospital-acquired infections increasingly involve multidrug-resistant Gram-negative pathogens.
Biofilm Formation: The Hidden Challenge
Biofilms represent one of the most strategically important aspects of recurrent and catheter-associated UTIs.
Biofilms are structured microbial communities enclosed within extracellular polymeric matrices.
Their development can conceptually be represented as:
\text{Planktonic bacteria} \rightarrow \text{Attachment} \rightarrow \text{Biofilm maturation}
Biofilms contribute to:
- Antibiotic tolerance
- Immune evasion
- Persistent infections
- Recurrent disease
Biofilm-associated infections may require:
- Catheter removal
- Combination therapy
- Extended treatment durations
Clinical Manifestations
Lower UTIs (Cystitis)
Symptoms include:
- Dysuria
- Urinary frequency
- Urgency
- Suprapubic pain
- Burning micturition
Upper UTIs (Pyelonephritis)
Kidney involvement may produce:
- Fever
- Flank pain
- Chills
- Nausea
- Sepsis
Pyelonephritis can become life-threatening if untreated.
Complicated and Severe Infections
Severe UTIs may lead to:
- Septic shock
- Acute kidney injury
- Multiorgan dysfunction
Hospitalized patients face particularly high morbidity.
Diagnostic Strategies
Modern UTI diagnosis increasingly integrates:
- Urinalysis
- Urine culture
- Molecular diagnostics
- Resistance profiling
- AI-assisted prediction systems
Traditional culture remains the gold standard.
However, culture-based diagnostics often require 48–72 hours.
Recent research highlights rapid urine testing technologies capable of predicting antibiotic susceptibility within hours rather than days. (The Pharmaceutical Journal)
AI-driven machine learning models are also being developed to predict resistance risk using electronic health record data. (CiplaMed)
Antimicrobial Resistance: The Central Crisis
Antimicrobial resistance has become the defining challenge in UTI management.
Recent global surveillance studies demonstrate rapidly rising resistance against:
- Fluoroquinolones
- Third-generation cephalosporins
- Trimethoprim-sulfamethoxazole
(PMC)
WHO data indicate that resistance among urinary pathogens is escalating worldwide. (World Health Organization)
The β-lactamase-mediated resistance mechanism may be represented conceptually as:
\beta\text{-lactam antibiotic} + \beta\text{-lactamase} \rightarrow \text{Inactive metabolite}
Major resistance mechanisms include:
- ESBL production
- Carbapenemases
- Efflux pumps
- Porin mutations
- Target-site modifications
India faces severe AMR challenges due to:
- OTC antibiotic use
- Empirical therapy misuse
- Inadequate stewardship
- High infectious burden
Recent Indian studies show rising resistance among UTI pathogens against fluoroquinolones and cephalosporins. (Journal of Pure and Applied Microbiology)
Conventional Treatment Strategies
Nitrofurantoin
Nitrofurantoin remains a frontline therapy for uncomplicated cystitis.
Advantages:
- High urinary concentration
- Lower systemic resistance
- Effective against many E. coli strains
Fosfomycin
Fosfomycin is increasingly used for:
- Multidrug-resistant UTIs
- ESBL-producing organisms
Its single-dose regimen improves compliance.
Trimethoprim-Sulfamethoxazole
Historically widely used, but resistance has increased substantially in many regions.
Fluoroquinolones
Examples:
- Ciprofloxacin
- Levofloxacin
These drugs possess excellent tissue penetration but are increasingly limited by resistance and safety concerns.
Cephalosporins
Third-generation cephalosporins remain important in complicated UTIs and pyelonephritis.
However, resistance against cephalosporins is increasing globally. (PMC)
Carbapenems
Carbapenems remain critical therapies for severe ESBL-associated infections.
However, carbapenem resistance is also emerging.
New Antibiotics and Therapeutic Innovations
Gepotidacin (Blujepa)
One of the most important recent developments is gepotidacin.
In 2025, the FDA approved gepotidacin for uncomplicated UTIs in females aged 12 years and older. (Sharp HealthCare)
Its importance lies in:
- Novel mechanism of action
- Activity against resistant strains
- First new oral UTI antibiotic class in decades
Gepotidacin inhibits bacterial topoisomerases using a mechanism distinct from fluoroquinolones.
Sulopenem
Sulopenem represents another promising oral therapy for resistant UTIs.
Recent studies demonstrated favorable outcomes in complicated UTIs. (MMITNetwork)
Pivmecillinam
Widely used in Europe for decades, pivmecillinam is gaining renewed attention due to effectiveness against resistant Gram-negative organisms. (MMITNetwork)
Non-Antibiotic Treatment Strategies
The future of UTI management increasingly involves reducing antibiotic dependency.
Immunomodulatory Therapies
Modern guidelines increasingly discuss immunomodulatory prophylaxis for recurrent UTIs. (Uroweb)
Vaccines
Researchers are developing vaccines targeting:
- UPEC adhesins
- Biofilm proteins
- Surface antigens
Intranasal vaccine research for UTI pathogens is also advancing. (CiplaMed)
Probiotics and Microbiome Therapy
Microbiome-based strategies aim to:
- Restore healthy microbial ecosystems
- Reduce pathogen colonization
- Prevent recurrence
Phage Therapy
Bacteriophage therapy is re-emerging as a promising strategy against multidrug-resistant uropathogens.
Precision Medicine and AI in UTI Management
Artificial intelligence is transforming infectious disease management.
AI systems are increasingly used for:
- Resistance prediction
- Personalized antibiotic selection
- Treatment optimization
- Epidemiological forecasting
Machine learning models now predict resistance risks using routine clinical variables. (CiplaMed)
Future precision medicine approaches may involve:
- Genomic resistance mapping
- Real-time susceptibility testing
- Personalized microbiome profiling
Catheter-Associated UTI Prevention
CAUTIs remain major hospital challenges.
Prevention strategies include:
- Limiting catheter use
- Aseptic insertion
- Antimicrobial-coated catheters
- Biofilm-resistant materials
- Strict infection control
Healthcare-associated infections significantly increase morbidity, mortality, and healthcare expenditure.
UTI Management in Special Populations
Pregnancy
UTIs during pregnancy increase risks of:
- Preterm labor
- Pyelonephritis
- Maternal complications
Safe antibiotic selection becomes critically important.
Elderly Patients
Aging populations exhibit:
- Higher recurrence
- Catheter dependence
- Polypharmacy interactions
Diabetic Patients
Hyperglycemia promotes bacterial growth and immune dysfunction.
Complicated infections are more common.
Pediatric UTIs
Children require careful evaluation due to:
- Risk of renal scarring
- Congenital abnormalities
- Long-term renal complications
Antimicrobial Stewardship
The future of UTI treatment depends heavily upon stewardship.
Core principles include:
- Culture-guided therapy
- Narrow-spectrum antibiotics
- Shorter treatment courses
- Avoiding unnecessary prescriptions
Recent guidelines increasingly support shorter antibiotic durations for many UTIs. (The Online GP)
Stewardship represents both:
- A scientific necessity
- An ethical responsibility
Industrial and Pharmaceutical Perspectives
The global UTI therapeutics market is expanding due to:
- Rising infection burden
- Aging populations
- Drug-resistant pathogens
- Demand for novel antibiotics
Pharmaceutical companies are increasingly investing in:
- Novel antibiotic classes
- Oral carbapenems
- Rapid diagnostics
- Combination therapies
The success of recent antibiotic approvals demonstrates renewed industrial interest in infectious disease therapeutics.
Future Outlook
The future of UTI management will likely be shaped by:
- Antimicrobial resistance escalation
- AI-driven diagnostics
- Precision infectious disease medicine
- Non-antibiotic therapies
- Microbiome engineering
- Vaccine development
- Rapid susceptibility testing
- Smart antimicrobial stewardship
Future UTI treatment may involve:
- Personalized antibiotic selection
- Real-time genomic diagnostics
- Biofilm-targeted therapies
- Microbiome restoration
- AI-guided antimicrobial decisions
The traditional empirical antibiotic model may gradually evolve into precision-guided infectious disease medicine.
Conclusion
Urinary tract infections represent far more than common bacterial illnesses.
They are now strategic indicators of:
- Global antimicrobial resistance
- Healthcare infrastructure quality
- Antibiotic stewardship effectiveness
- Pharmaceutical innovation capacity
- Precision medicine evolution
The modern UTI landscape reflects an ongoing battle between microbial adaptation and human scientific progress.
On one side stand:
- Drug-resistant pathogens
- Biofilm biology
- Healthcare-associated infections
- Antibiotic misuse
On the other side stand:
- Novel antibiotics
- AI-driven diagnostics
- Precision medicine
- Vaccine science
- Synthetic biology
- Antimicrobial stewardship
The emergence of new therapies such as gepotidacin demonstrates that innovation in infectious disease medicine is still possible. (Reuters)
However, no antibiotic alone can solve the UTI crisis.
Long-term success will require integrated coordination among:
- Clinicians
- Pharmacologists
- Microbiologists
- Policymakers
- Pharmaceutical industries
- Public health agencies
- Patients themselves
In the coming decades, urinary tract infections may become one of the defining battlegrounds of the global antimicrobial resistance era.
How humanity responds to this challenge will shape not only the future of infectious disease medicine, but the future sustainability of modern healthcare itself.