
Understanding the Biological Complexity and Therapeutic Management of Ulcerative Disorders
Introduction
Ulcers represent one of the most significant pathological manifestations encountered across multiple organ systems in human medicine. Fundamentally, an ulcer refers to a localized discontinuity or breakdown of epithelial or mucosal tissue accompanied by inflammation, necrosis, and impaired healing processes. Although ulcers are commonly associated with the gastrointestinal tract, ulcerative disorders can affect numerous tissues including the skin, oral cavity, cornea, vascular systems, and mucosal linings. The pathogenesis of ulcers involves a highly complex interaction among inflammatory mediators, oxidative stress, microbial invasion, ischemia, immune dysregulation, cellular apoptosis, vascular dysfunction, and impaired regenerative signaling pathways.
The global burden of ulcerative diseases remains substantial. Peptic ulcer disease, diabetic foot ulcers, pressure ulcers, venous ulcers, oral ulcers, and inflammatory bowel-associated ulcerations contribute significantly to morbidity, healthcare expenditure, hospitalization rates, and reduced quality of life. In developing nations such as India, ulcerative disorders are further aggravated by delayed diagnosis, nutritional deficiencies, infectious diseases, irrational drug use, poor glycemic control, smoking, alcohol consumption, and limited healthcare accessibility.
Historically, ulcers were primarily attributed to excessive acid secretion and local tissue injury. However, modern molecular biology has revealed that ulcer formation is governed by intricate cellular signaling networks involving:
- Nuclear factor-kappa B (NF-κB)
- Cyclooxygenase pathways
- MAPK signaling
- PI3K/Akt pathways
- Cytokine cascades
- Oxidative stress mechanisms
- Hypoxia-induced pathways
- Growth factor dysregulation
- Apoptotic signaling systems
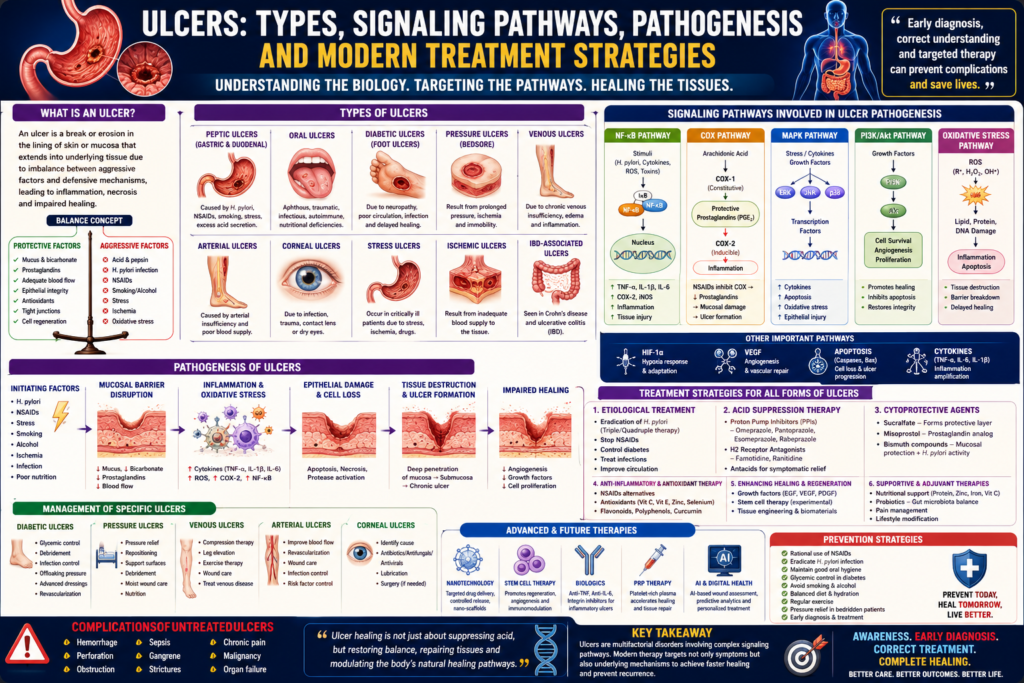
The understanding of these signaling pathways has revolutionized ulcer therapeutics. Modern treatment strategies no longer focus solely upon symptomatic acid suppression or wound covering. Instead, contemporary medicine increasingly aims to:
- Modulate inflammatory pathways
- Restore epithelial integrity
- Enhance angiogenesis
- Promote tissue regeneration
- Correct microbial dysbiosis
- Reduce oxidative injury
- Improve immune regulation
This article presents a comprehensive and structured discussion regarding the major types of ulcers, molecular signaling pathways involved in ulcer pathogenesis, pathological mechanisms, and advanced therapeutic strategies for the management of ulcerative diseases.
Understanding Ulcers: Basic Definition and Pathophysiology
An ulcer is defined as a breach or erosion in the epithelial surface extending into underlying tissues due to destruction of protective cellular barriers. Unlike superficial erosions, ulcers involve deeper tissue damage accompanied by inflammatory responses and delayed healing.
Normal tissue integrity depends upon a balance between:
- Protective mechanisms
and - Aggressive injurious factors
When destructive influences exceed tissue defense capacity, ulceration develops.
Protective mechanisms include:
- Mucus secretion
- Bicarbonate production
- Adequate blood flow
- Tight junction integrity
- Cellular regeneration
- Antioxidant systems
- Growth factor signaling
Aggressive factors include:
- Acid secretion
- Proteolytic enzymes
- Reactive oxygen species
- Ischemia
- Microbial toxins
- Mechanical trauma
- Inflammatory cytokines
Ulcer formation therefore reflects failure of tissue homeostasis.
Classification and Types of Ulcers
Ulcers may be classified according to anatomical location, etiological mechanism, pathological characteristics, or underlying disease associations.
Major ulcer categories include:
- Peptic ulcers
- Gastric ulcers
- Duodenal ulcers
- Oral ulcers
- Diabetic ulcers
- Pressure ulcers
- Venous ulcers
- Arterial ulcers
- Corneal ulcers
- Stress ulcers
- Ischemic ulcers
- Inflammatory bowel disease-associated ulcers
Peptic Ulcer Disease
Overview
Peptic ulcer disease (PUD) represents one of the most extensively studied ulcerative disorders. It involves ulceration within gastric or duodenal mucosa due to imbalance between aggressive acid-peptic activity and mucosal defense systems.
Major causes include:
- Helicobacter pylori infection
- NSAID use
- Stress
- Smoking
- Alcohol consumption
- Hypersecretory states
Gastric Ulcers
Gastric ulcers occur primarily within the stomach lining.
Pathogenesis involves:
- Mucosal barrier disruption
- Reduced prostaglandin synthesis
- Oxidative stress
- Local ischemia
- Acid-mediated tissue injury
Symptoms include:
- Epigastric pain
- Nausea
- Vomiting
- Weight loss
- Gastrointestinal bleeding
Duodenal Ulcers
Duodenal ulcers are more commonly associated with excessive acid secretion and Helicobacter pylori colonization.
They frequently present with:
- Burning abdominal pain
- Nocturnal discomfort
- Relief after meals
Unlike gastric ulcers, duodenal ulcers often involve hyperchlorhydria.
Oral Ulcers
Oral ulcers include:
- Aphthous ulcers
- Traumatic ulcers
- Infectious ulcers
- Autoimmune ulcerations
Contributing factors include:
- Nutritional deficiencies
- Stress
- Immune dysregulation
- Viral infections
- Systemic inflammatory disorders
Diabetic Foot Ulcers
Diabetic ulcers represent one of the most devastating complications of diabetes mellitus.
Pathogenesis involves:
- Peripheral neuropathy
- Microvascular dysfunction
- Impaired immunity
- Chronic inflammation
- Delayed wound healing
These ulcers significantly increase amputation risk.
Pressure Ulcers
Pressure ulcers, also called bedsores, result from prolonged pressure-induced ischemia.
Risk factors include:
- Immobility
- Malnutrition
- Neurological disorders
- Advanced age
Tissue hypoxia and impaired perfusion play central roles.
Venous and Arterial Ulcers
Venous Ulcers
Venous ulcers arise from chronic venous insufficiency leading to:
- Venous hypertension
- Edema
- Inflammatory injury
Arterial Ulcers
Arterial ulcers occur due to ischemia caused by:
- Peripheral arterial disease
- Atherosclerosis
- Reduced tissue perfusion
Corneal Ulcers
Corneal ulcers involve inflammatory destruction of corneal tissue.
Causes include:
- Bacterial infections
- Fungal infections
- Trauma
- Contact lens misuse
Vision-threatening complications may occur.
Molecular Signaling Pathways in Ulcer Pathogenesis
Modern ulcer biology emphasizes complex intracellular signaling cascades that regulate inflammation, apoptosis, oxidative stress, angiogenesis, and tissue repair.
NF-κB Signaling Pathway
The NF-κB pathway represents one of the central inflammatory signaling mechanisms involved in ulcerogenesis.
Under pathological conditions:
- Reactive oxygen species
- Cytokines
- Bacterial toxins
activate NF-κB signaling.
This results in increased expression of:
- TNF-α
- IL-1β
- IL-6
- COX-2
- Adhesion molecules
Excessive NF-κB activation promotes:
- Chronic inflammation
- Tissue destruction
- Delayed healing
In Helicobacter pylori-associated ulcers, bacterial virulence factors strongly activate NF-κB-mediated inflammation.
Cyclooxygenase (COX) Pathway
Cyclooxygenase enzymes regulate prostaglandin synthesis.
COX-1
COX-1 supports:
- Mucosal protection
- Bicarbonate secretion
- Gastric blood flow
COX-2
COX-2 becomes induced during inflammation.
NSAIDs inhibit COX enzymes, reducing protective prostaglandin levels and increasing ulcer risk.
MAPK Signaling Pathway
Mitogen-activated protein kinase (MAPK) signaling regulates:
- Cellular stress responses
- Inflammation
- Apoptosis
Major MAPK subtypes include:
- ERK
- JNK
- p38 MAPK
Activation contributes to:
- Cytokine production
- Epithelial injury
- Oxidative damage
PI3K/Akt Signaling Pathway
The PI3K/Akt pathway plays critical roles in:
- Cell survival
- Angiogenesis
- Tissue regeneration
Impaired PI3K/Akt signaling contributes to:
- Delayed wound healing
- Increased apoptosis
- Impaired epithelial repair
Activation of this pathway promotes ulcer healing.
Oxidative Stress Pathways
Oxidative stress represents a major pathological mechanism in ulcer formation.
Reactive oxygen species damage:
- Lipids
- Proteins
- DNA
- Cell membranes
Major oxidative mediators include:
- Superoxide radicals
- Hydrogen peroxide
- Hydroxyl radicals
Oxidative stress further activates inflammatory cascades and apoptosis.
Hypoxia-Inducible Factor (HIF) Pathway
Hypoxia is particularly important in:
- Pressure ulcers
- Diabetic ulcers
- Ischemic ulcers
HIF signaling regulates:
- Angiogenesis
- Cellular adaptation to hypoxia
- VEGF production
Disrupted HIF signaling impairs tissue repair.
VEGF and Angiogenesis Signaling
Vascular endothelial growth factor (VEGF) is essential for:
- Neovascularization
- Wound healing
- Tissue regeneration
Reduced VEGF activity contributes to chronic non-healing ulcers.
Apoptotic Signaling Pathways
Excessive apoptosis contributes to ulcer progression.
Key mediators include:
- Caspases
- Bax proteins
- Mitochondrial dysfunction
Uncontrolled epithelial apoptosis weakens mucosal integrity.
Role of Helicobacter pylori in Peptic Ulcer Pathogenesis
Helicobacter pylori revolutionized understanding of peptic ulcer disease.
The bacterium:
- Produces urease
- Disrupts mucosal barriers
- Induces inflammation
- Activates NF-κB pathways
- Generates oxidative stress
Virulence factors such as:
- CagA
- VacA
contribute significantly to tissue injury.
Chronic infection increases risk of:
- Gastric ulcers
- Duodenal ulcers
- Gastric cancer
NSAID-Induced Ulcers
NSAIDs inhibit prostaglandin synthesis through COX inhibition.
Consequences include:
- Reduced mucus secretion
- Decreased bicarbonate production
- Impaired blood flow
- Increased acid-mediated injury
Common ulcerogenic NSAIDs include:
- Aspirin
- Diclofenac
- Ibuprofen
- Naproxen
Stress and Neuroendocrine Factors in Ulcers
Psychological stress influences ulcer development through:
- Cortisol elevation
- Sympathetic activation
- Reduced mucosal perfusion
- Increased oxidative stress
Severe physiological stress may produce stress ulcers in critically ill patients.
Modern Treatment Strategies for Ulcers
Ulcer management now involves:
- Etiological treatment
- Symptom control
- Inflammation suppression
- Tissue regeneration
- Prevention of recurrence
Proton Pump Inhibitors (PPIs)
PPIs remain first-line therapy for acid-related ulcers.
Common agents include:
- Omeprazole
- Pantoprazole
- Esomeprazole
Mechanism:
- Irreversible inhibition of H+/K+ ATPase
Benefits include:
- Acid suppression
- Mucosal healing
- Reduced bleeding risk
H2 Receptor Antagonists
Agents such as:
- Ranitidine
- Famotidine
reduce gastric acid secretion through histamine receptor blockade.
Antibiotic Therapy for Helicobacter pylori
Eradication regimens include:
- PPIs
- Clarithromycin
- Amoxicillin
- Metronidazole
Triple or quadruple therapy is commonly employed.
Cytoprotective Agents
Sucralfate
Sucralfate forms protective barriers over ulcers.
Misoprostol
Misoprostol restores prostaglandin-mediated mucosal protection.
Useful particularly in NSAID-induced ulcers.
Antioxidant Therapy
Oxidative stress modulation is increasingly recognized.
Potential antioxidants include:
- Vitamin C
- Vitamin E
- Polyphenols
- Flavonoids
Experimental therapies target ROS reduction.
Growth Factor Therapy
Growth factors such as:
- VEGF
- EGF
- PDGF
promote:
- Angiogenesis
- Cellular proliferation
- Tissue repair
Particularly useful in chronic wounds.
Stem Cell Therapy
Stem cell approaches are emerging for chronic non-healing ulcers.
Potential mechanisms include:
- Regenerative signaling
- Immunomodulation
- Enhanced angiogenesis
Research remains ongoing.
Biological Therapies and Cytokine Modulation
Biologics targeting inflammatory cytokines are increasingly used in:
- Inflammatory bowel disease-associated ulcers
- Autoimmune ulcerative disorders
Targets include:
- TNF-α
- IL-6
- Integrin signaling
Diabetic Ulcer Management
Comprehensive diabetic ulcer care includes:
- Glycemic control
- Debridement
- Infection management
- Pressure offloading
- Vascular optimization
Advanced wound dressings and regenerative therapies are increasingly employed.
Pressure Ulcer Treatment
Management includes:
- Pressure redistribution
- Nutritional support
- Debridement
- Moist wound healing
- Infection prevention
Venous Ulcer Therapy
Key strategies include:
- Compression therapy
- Venous insufficiency management
- Wound care
- Surgical correction when necessary
Corneal Ulcer Management
Therapy depends upon etiology.
Treatments include:
- Antibiotics
- Antifungals
- Antivirals
- Corticosteroids in selected cases
Prompt intervention prevents vision loss.
Role of Nutrition in Ulcer Healing
Nutrition significantly influences tissue repair.
Important nutrients include:
- Proteins
- Zinc
- Vitamin C
- Arginine
- Iron
Malnutrition delays ulcer healing substantially.
Herbal and Natural Therapies
Several herbal agents exhibit anti-ulcer properties.
Examples include:
- Curcumin
- Aloe vera
- Licorice
- Honey extracts
Potential mechanisms involve:
- Antioxidant activity
- Anti-inflammatory effects
- Enhanced regeneration
However, rigorous clinical validation remains necessary.
Nanotechnology and Future Ulcer Therapies
Nanomedicine offers promising future approaches including:
- Targeted drug delivery
- Controlled-release systems
- Nano-scaffolds
- Regenerative biomaterials
Nanotechnology may revolutionize chronic ulcer treatment.
Artificial Intelligence and Ulcer Management
AI applications include:
- Wound assessment
- Predictive healing models
- Risk stratification
- Personalized therapy optimization
Digital healthcare integration is expected to improve ulcer care substantially.
Prevention Strategies
Ulcer prevention remains critically important.
Preventive approaches include:
- Rational NSAID use
- Helicobacter pylori eradication
- Glycemic control
- Smoking cessation
- Nutritional optimization
- Pressure redistribution in immobilized patients
Preventive medicine significantly reduces ulcer burden.
Complications of Untreated Ulcers
Untreated ulcers may cause:
- Hemorrhage
- Perforation
- Sepsis
- Gangrene
- Malignancy
- Organ dysfunction
Early intervention is therefore essential.
Conclusion
Ulcers represent highly complex pathological disorders involving intricate interactions among inflammatory pathways, oxidative stress mechanisms, immune responses, vascular dysfunction, microbial invasion, and impaired tissue regeneration. Modern understanding of ulcer biology has evolved far beyond simplistic concepts of acid injury and tissue erosion. Today, ulcerative diseases are increasingly recognized as multifactorial molecular disorders governed by highly sophisticated signaling networks including NF-κB, MAPK, PI3K/Akt, COX, VEGF, oxidative stress cascades, and apoptotic pathways.
The diversity of ulcerative disorders — ranging from peptic ulcers and diabetic foot ulcers to pressure ulcers and inflammatory mucosal lesions — reflects the broad systemic importance of tissue integrity and wound healing mechanisms in human physiology.
Contemporary therapeutic strategies are progressively transitioning toward:
- Precision medicine
- Regenerative therapies
- Molecular targeting
- Immunomodulation
- Growth factor enhancement
- Nanotechnology-driven drug delivery
The future of ulcer management will likely involve integrated multidisciplinary approaches combining:
- Pharmacology
- Biotechnology
- Molecular medicine
- Artificial intelligence
- Tissue engineering
- Personalized therapeutics
India and other developing nations face substantial ulcer-related healthcare burdens due to rising diabetes prevalence, aging populations, irrational NSAID use, infectious diseases, malnutrition, and healthcare disparities. Therefore, future healthcare systems must prioritize:
- Early diagnosis
- Preventive medicine
- Patient education
- Research innovation
- Affordable therapeutic accessibility
The scientific understanding of ulcer pathogenesis continues to expand rapidly, opening new opportunities for targeted intervention and regenerative healing strategies.
The future management of ulcers will no longer focus merely upon symptom suppression.
The future of ulcer therapeutics will focus upon restoring molecular balance, regenerative integrity, and long-term tissue resilience at the cellular and signaling pathway level itself.